The mechanisms and pathways involved in the health and aging benefits conveyed by green tea were investigated in C. elegans.
The Trending With Impact series highlights Aging (Aging-US) publications that attract higher visibility among readers around the world online, in the news, and on social media—beyond normal readership levels. Look for future science news about the latest trending publications here, and at Aging-US.com.
—
Listen to an audio version of this article
Boiled or iced with water or milk, blended in smoothies, condensed into shots or even baked into pastries—humans are infatuated with green tea. Today, green tea is one of the most widely consumed beverages in the world. Molecules found in this plant, named catechins, are known to have numerous evidence-based health benefits, including weight loss and age delaying properties. However, the mechanism by which these effects take place have yet to be fully elucidated.
“The popularity of green tea makes it crucial to study its impact on health and aging.”
“We have designed the current study to investigate the impact and to unveil the target of the most abundant green tea catechins, epigallocatechin gallate (EGCG) and epicatechin gallate (ECG).”
The Study
In this study, the researchers focused on testing two of the most common green tea catechins, epigallocatechin gallate (EGCG) and epicatechin gallate (ECG), in isolated mitochondria from murine liver and C. elegans. C. elegans are approximately one millimeter long nematodes, or roundworms, and have been used in a variety of biomedical studies. The reason C. elegans were chosen for this study is likely due to the fact that many genes in C. elegans have functional counterparts in humans. (C. elegans also have the ability to “smell” cancer.)
Over the course of 24 hours or seven days, C. elegans and rodent mitochondria were treated with 2.5 μM of EGCG and/or ECG compounds. To analyze the green tea catechins’ effects on cellular metabolism, reactive oxygen species (ROS) homeostasis, stress resistance, physical exercise capacity, health- and lifespan, and on the underlying signaling pathways, the researchers conducted lifespan analyses, locomotion assay, paraquat stress resistance assay, basal oxygen consumption rate, ROS quantification, glucose oxidation assay, ATP quantification, activity assays for catalase and superoxide dismutase, fat content analysis, quantification of complex I activity in mitochondria, quantification of oxygen consumption rate in mitochondria, and statistical analyses.
“We conclude that applying the green tea catechins EGCG and ECG at a low dose extends the lifespan of C. elegans via inducing a mitohormetic response.”
They found that the catechins hindered mitochondrial respiration in C. elegans after 6–12 hours, the activity of complex I in isolated rodent mitochondria and temporarily increased ROS levels. Then, after 24 hours and through adaptive responses, catechins reduced fat content, enhanced ROS defense and, in the long term, improved healthspan in C. elegans.
Conclusion
Mechanisms and pathways observed to be involved in this process of C. elegans fitness and lifespan extension by green tea were further described in the paper. The researchers note that additional studies will be required to determine the best timing and dosage for administering catechins. They also acknowledge that the low bioavailability of green tea catechins may limit the lifespan extending effects of green tea in humans, despite the promising effects demonstrated in C. elegans.
“Despite the promising results obtained in animal experiments, the low bioavailability of EGCG [7] still raises the question of whether green tea catechins can reliably provoke beneficial effects in humans. Consequently, additional efforts might be needed to identify complex I inhibitors with increased bioavailability.”
Click here to read the full priority research paper published by Aging (Aging-US).
Aging (Aging-US) is an open-access journal that publishes research papers monthly in all fields of aging research and other topics. These papers are available to read at no cost to readers on Aging-us.com. Open-access journals offer information that has the potential to benefit our societies from the inside out and may be shared with friends, neighbors, colleagues, and other researchers, far and wide.
Researchers adopted 103 retired sled dogs for a longitudinal study on canine aging that may one day be used to increase human healthspan and longevity.
The Trending With Impact series highlights Aging (Aging-US) publications that attract higher visibility among readers around the world online, in the news, and on social media—beyond normal readership levels. Look for future science news about the latest trending publications here, and at Aging-US.com.
—
Listen to an audio version of this article
Whether they are sprinters or distance runners, sled dogs are known for their competitive nature and athletic prowess. With age, however, these athletes eventually run out of steam—just as humans inevitably do. Canines of all breeds are affected by aging, including a loss of resilience, accumulation of molecular damage and age-related diseases. These relatively short-lived, large mammals are one of the few to share environments with humans, and even have access to advanced medical care. Many believe the canine aging process resembles human aging the closest compared to any other animal.
The researchers chose to adopt retiredsleddogs for this study in particular for a variety of reasons: 1) Based on the type of events they partake in, sled dogs usually have a record of health and performance that can be used for reference as they age. 2) Sled dogs are selected for performance, but are not limited to a particular breed and can be crossbred. This provides a somewhat homogeneous population to study while being less prone to breed-specific biases. 3) Sled dogs are used to working with many handlers, therefore, the transition into the kennel/research facility may be easier for them to adjust to. 4) Over their career, these dogs have been exposed to environmental pathogens in frequent group interactions. This provides the researchers a sufficient immune system model to study. 5) Sled dogs are used to living in packs, but forming short-term bonds—making them adaptable to living with a variety of handlers in a population of 103 other dogs.
“Thus, it is essential to establish a reference set of ‘healthy aging’ parameters specifically for each dog model, and we see this as one of the main goals of our sled dog study.”
The optics of caring for 103 retired sled dogs between the ages of eight and 11 (when the study began) may initially sound problematic, but all indications suggest that these dogs are living better than many humans. Their 8,254-square foot kennel is located on the Baker Institute campus of the College of Veterinary Medicine at Cornell University. The researchers designed the study so that the dogs are thoroughly examined, observed, fed, socialized, exercised, vaccinated and anything else they may need. The dogs’ personalities and special needs are taken into consideration when cohabitating with other dogs, in their separate rooms and during playtime outside. They have in-house veterinarians and researchers to monitor their health. Importantly, the researchers are monitoring not only the dogs’ health but also parameters of their individual aging experience.
“Our goal is not just to assess the state of health of a given dog but rather to dissect the aging process into its two key components: (i) declining resilience and (ii) acquisition of aging-related diseases.”
In order to observe declining resilience and aging-related diseases, the dogs participate in regular physical fitness (treadmill and pull tests) and cognitive tests (handler questionnaires, β-amyloid plaques, brain atrophy, neuron loss, and etc.). Their performance and scores are measured and compared to their previous scores. The researchers also regularly collect blood samples to assess the dogs for somatic cell genome modifications (accumulation of DNA damage) and immune system status (immunosenescence).
“In general, the canine immune system undergoes similar age-related changes to that of humans [85]. However, since completed canine studies are generally less comprehensive and predominantly cross-sectional, the reliability and relative significance of various immune parameters in aging have yet to be characterized.”
CONCLUSION
This research is still ongoing, and the researchers believe the infrastructure they established in this sled dog study is an important advancement in aging research. In the future, this animal model may be used to test anti-aging therapies and translate into advancing human healthspan and lifespan.
“We expect that these analyses will allow us to (i) characterize the mechanism(s) and regulation of canine aging, (ii) identify parameters and biomarkers suitable for assessment of biological age, and (iii) define factors that may act as aging accelerators or decelerators.”
Click hereto read the full research perspective, published by Aging (Aging-US).
Aging (Aging-US) is an open-access journal that publishes research papers twice a month—in all fields of aging research and other biomedical topics. These papers are available to read at no cost to readers on Aging-us.com. Open-access journals offer information that has the potential to benefit our societies from the inside out and may be shared with friends, neighbors, colleagues, and other researchers, far and wide.
In June 2021, Web of Science (Clarivate Analytics) released their 2020 JCR Impact Factor. Aging‘s 2020 impact factor is 5.682.
Listen to an audio version of this announcement
BUFFALO, NY-August 20, 2021 – Agingis indexed by Web of Science: Science Citation Index Expanded (abbreviated as Aging‑US). In June 2021, Web of Science (Clarivate Analytics) released their 2020 JCR Impact Factor. Aging is pleased to report that our 2020 impact factor is 5.682. This number has increased from last year’s 4.831. Without self-citation, Aging’s 2020 impact factor is 5.279.
Aging is listed in the Web of Science: Science Citation Index Expanded in two categories: Cell Biology and Geriatrics & Gerontology. According to the Journal Citation Indicator (JCI), Aging is ranked in the Q1 quartile in both categories.
Since 2009, Aginghaspublished research papers in all fields of aging research including, but not limited to, aging from yeast to mammals, cellular senescence, age-related diseases such as cancer and Alzheimer’s diseases and their prevention and treatment, anti-aging strategies and drug development and especially the role of signal transduction pathways such as mTOR in aging and potential approaches to modulate these signaling pathways to extend lifespan.
This journal aims to promote treatment of age-related diseases by slowing down aging, validation of anti-aging drugs by treating age-related diseases, and prevention of cancer by inhibiting aging. Cancer and COVID-19 are age-related diseases.
To learn more about Aging, publication standards, and past or current issues, visit www.aging-us.com.
Impact Journals is an open-access publisher of research journals in biomedical sciences. Our publications focus on topics surrounding cancer research and all fields of aging research. Our mission is to provide scientists with the opportunity to share their exceptional discoveries, offer services that enable rapid dissemination of results, and to present vital findings from the many fields of biomedical science.
The MEND (Bredesen) protocol to treat neurodegeneration associated with Alzheimer’s disease was tested in a small cohort. In 2016, researchers followed up with objective results.
Blue synapse and neuron. 3D rendering
The Top-Performer series highlights papers published by Agingthat have generated a high Altmetric Attention score. Altmetric scores, located at the top-left of trending Aging papers, provide an at-a-glance indication of the volume and type of online attention the research has received.
Precursors to the onset of early Alzheimer’s disease (AD) include mild cognitive impairment (MCI) and subjective cognitive impairment (SCI). Many have viewed this looming neurodegeneration as an unavoidable fate that accompanies aging. However, in a 2014 study, a novel precision medicine treatment approach, termed the metabolic enhancement for neurodegeneration (MEND) protocol, yielded unprecedented results. Nine out of 10 participants with memory loss associated with AD, amnestic MCI, and SCI, were treated using the MEND protocol. Participants displayed subjective improvement in cognition within 3-6 months of this protocol. The study claims their only failure was one patient with very late stage AD.
“In each of these cases, obvious subjective improvement, noted by the patient, his/her significant other, and his/her co-workers, was accompanied by clear, quantitated, objective improvement.”
THE MEND PROTOCOL
The MEND protocol, also known as the Bredesen Protocol (named after the creator of the protocol, Dr. Dale Bredesen), consists of a multifaceted, tailored approach to treating each AD patient for their individual symptoms of cognitive decline—and not only a few symptoms. This strategy uses a combination of diet, lifestyle, and therapeutic interventions. Treatment is based on the hypothesis that AD occurs due to an imbalance in an extensive plasticity network in the brain. The authors note that the MEND protocol is an iterative process and designed to improve with continued patient visits.
“The therapeutic system described in this report derives from basic studies of the role of APP signaling and proteolysis in plasticity, and the imbalance in this receptor proteolysis that reproducibly occurs in Alzheimer’s disease.”
Upon clinical assessment and lab testing, the patients’ physical and cognitive health were evaluated. Based on this assessment, patients were prescribed a lengthy personalized therapeutic system. Among other objectives, the MEND protocol recommends treating diabetes; improving sleep and digestive health; reducing stress, inflammation, and blood sugar; increasing physical exercise, intellectual stimulation, antioxidants, and vitamins; and optimizing hormone balance, synthesis of acetylcholine, nerve growth factors and mitochondrial function.
ANECDOTAL AND OBJECTIVE RESULTS
“The magnitude of the improvement is unprecedented, providing additional objective evidence that this programmatic approach to cognitive decline is highly effective.”
Before participating in the MEND protocol, most of the 10 participants reported a family history of AD, confusion, difficulty with word finding, following instructions, remembering, reading, concentrating, driving, completing work related tasks, and other cognitive struggles. Over the course of between five and 24 months on the MEND, nine of 10 patients and their families or caregivers reported improved cognitive function. Some patients were able to go back to work, play games, and even babysit their grandchildren. One spouse of a patient mentioned that her husband had stopped following the protocol for a period of time, which resulted in him leaving the car in the driveway idling with the keys in the ignition. After he resumed the protocol, no such instances were reported.
Bearing in mind that this study used an extremely small cohort to test this very expensive protocol, the objective results observed by the researchers were still considerably significant. Quantitative neuropsychological testing showed improvements of up to three standard deviations. One patient showed an increase in hippocampal volume from 17th percentile to 75th percentile. These results must be verified in a larger sample size to validate efficacy.
CONCLUSION
“The initial results for these patients show greater improvements than have been reported for other patients treated for Alzheimer’s disease. The results provide further support for the suggestion that such a comprehensive approach [3] to treat early Alzheimer’s disease and its precursors, MCI and SCI, is effective. The results also support the need for a large-scale, personalized clinical trial using this protocol.”
Click here to read the full research paper, published by Aging.
Aging is an open-access journal that publishes research papers monthly in all fields of aging research and other topics. These papers are available to read at no cost to readers on Aging-us.com. Open-access journals offer information that has the potential to benefit our societies from the inside out and may be shared with friends, neighbors, colleagues, and other researchers, far and wide.
From the University of California Berkeley and Apheresis Care Group, researchers discovered a method of “refreshing” blood that reverses some of the effects of aging.
Infusion drips with bottles of yellow albumin fluid.
The Top-Performer series highlights papers published by Aging that have generated a high Altmetric attention score. Altmetric scores, located at the top-left of trending Aging papers, provide an at-a-glance indication of the volume and type of online attention the research has received.
Is it possible for old blood to be “refreshed” in order to rejuvenate youth and combat the effects of aging? Aging researchers have a long history of analyzing the blood in search of the keys to healthy aging. In 2020, researchers from the University of California Berkeley and Apheresis Care Group uncovered groundbreaking new insights about the rejuvenation of aging blood with the potential to slow, and potentially to reverse, aging. Their well-read priority research paper was published by Aging and entitled, “Rejuvenation of three germ layers tissues by exchanging old blood plasma with saline-albumin.” To date, this top-performing paper has generated an impressive Altmetric Attention score of 147.
Blood Plasma
Approximately 55% of the body’s total blood volume is composed of a pale yellow liquid—plasma. Plasma largely consists of water (about 92%), with traces of mineral salts, sugars, fats, hormones, and vitamins. This watery substance also contains important proteins, such as immunoglobulin (antibodies), clotting/coagulation factors, and albumin.
“In people, albumin levels correlate with disease, nutrition, and socio-economic status rather than chronological age; and even when health, etc. status are not considered, albumin diminishes only marginally, by 2-4% at 75 years of age from its 26 years of age levels [21–24].”
Plasmapheresis is a general term used to describe procedures that remove, treat, and return or exchange blood plasma to the blood. Patients with autoimmune diseases, sickle cell disease, certain forms of neuropathy, and even severe cases of malaria have benefitted from plasmapheresis.
Heterochronic Parabiosis
Heterochronic parabiosis, a plasmapheresis-like procedure, is the surgical joining of two organisms in an effort to study the physiological changes that result from shared blood flow. Researchers have used this model of joining young and old animals together to observe the effects of old blood in young mice, and vice versa. In a 2005 study, University of California Berkeley and Apheresis Care Group researchers found that, through the process of heterochronic parabiosis, old mice sharing blood with young mice produced rejuvenating effects in old mice.
“The general conclusion of these studies was that the old partners had better health and/or repair of cartilage, muscle, liver, brain, spinal cord, kidneys, bone, skin, etc., and often the young animals experienced premature aging of their respective tissues [1, 3, 4, 6–8].”
However, the same researchers suspected that the rejuvenating effects demonstrated by heterochronic parabiosis were not direct results of youthful factors in the young murine blood itself. They also suspected that the premature aging experienced by the young mice were not due to old factors in the aged blood either. The team proposed that simply diluting the young and old factors in the blood may be the cause of these effects. In 2020, the researchers conducted a new study, this time using saline and albumin, to test their hypothesis.
“Historically, the phenomena of heterochronic parabiosis and blood exchange remained unconfirmed with respect to the key assumption as to whether the addition of young factors is needed for rejuvenation, and if premature aging of young mice stemmed from the introduction of old blood factors or a simple dilution of young factors.”
The Study
In this study, the researchers began by conducting a plasmapheresis procedure in mice called a neutral blood exchange (NBE). Half of the platelet-rich-plasma (PRP) was removed from the blood in young and old mice and was replaced with a simple saline and 5% purified albumin.
“Through a half-hour long series of small volume exchanges, 50% of the PRP of old and young mice was replaced with saline plus 5% mouse albumin while the circulating red and white blood cells were returned isochronically to the animal.”
Their results showed that a single session of NBE improved regeneration, reduced fibrosis, enhanced myogenesis, and other factors in the old mice. In the young mice, they found that this procedure did not have adverse effects or worsen the aforementioned factors. To verify their findings, the team studied human blood samples from four older individuals (between the ages 65 and 70) and conducted an FDA approved procedure, Therapeutic Plasma Exchange (TPE), using the same saline/albumin formula.
“To confirm these findings and to explore their evolutionary conservation, we took advantage of the fact that there is a procedure for human patients analogous to NBE, where most of the plasma is replaced by physiologic solution supplemented with commercial human albumin, called Therapeutic Plasma Exchange, TPE, which is FDA approved and routinely used in the clinic [16–18].”
Conclusion
In summary, their research found that simply diluting old blood factors with a neutral substance such as saline and albumin contributes to improving muscle repair, attenuating fibrosis, enhancing myogenic proliferation, reducing liver adiposity and fibrosis, and increasing hippocampal neurogenesis. In some areas, they found that these effects were even stronger in TPE than results after heterochronic parabiosis or blood exchange.
“The theoretical significance of this study is in a better understanding of how blood heterochronicity acts to quickly and profoundly rejuvenate old mammals, and the clinical significance of this work is in developing TPE as a new modality to broadly improve organ health and repair in older individuals preventing illnesses that develop or become more severe in later decades of life.”
Click here to read the full priority research paper, published by Aging.
Aging is an open-access journal that publishes research papers monthly in all fields of aging research and other topics. These papers are available to read at no cost to readers on Aging-us.com. Open-access journals offer information that has the potential to benefit our societies from the inside out and may be shared with friends, neighbors, colleagues, and other researchers, far and wide.
Behind the Study is a series of transcribed videos from researchers elaborating on their recent oncology-focused studies published by Aging. Visit the AgingYouTube channel for more insights from outstanding authors.
—
It’s David Sinclair here. I’m talking to you from my home in Boston during this pandemic stayed home time, but also wanted to talk to you about a new paper that we have coming out, or just came out in our journal, Aging, and its title is, “Why Does COVID-19 Disproportionately Affect the Elderly?”—which has become one of the biggest questions I think in this whole pandemic. And, if we could understand why the elderly were more susceptible, first of all, we could help them survive and have less severe cases, but also we could learn perhaps why younger people are also more susceptible. One thing that I often hear when I pose that question is oh, it’s just that old people are sicker and they die. Well, that’s not a good enough explanation because the elderly, even if they are healthy, have a much greater chance of dying than someone whose say, less than 65.
In fact, of all the main causes of death or risk factors in COVID-19, age is by far the most important one, independent of all those other risk factors. So a study just came out in the UK that looked at 17 million people that had COVID-19 and they could tell us based on that, what the ranking of the what’s called the hazard ratio of which symptoms and which lifestyle and cobalt morbidities track with COVID-19 more fatality risk.
And actually, in order starting with number five, it was diabetes/obesity. Number three was being male, that’s fairly risky. Having cancer of the blood was bad, which makes sense because you’ve disrupted your immune system. But by far the riskiest thing is age, independent of all these other things. In fact, compared to these other risks, age is basically the major determinate. If you’re 80, numbers where you’re about tenfold higher to someone who’s in their late 50s. So that led us to try to figure out what is going on with the age that makes them more susceptible. And again, it’s not just that those people start out sicker. And so we’ve written this perspective and gathered a lot of data from around the world, papers that have come out, papers that have been in publication. So in this perspective, we’ve gathered a lot of data from around the world, new papers, old papers, and really put together a list of things that we think are the most likely explanations for the elderly succumbing to COVID-19, independent of their actual underlying diseases and frailty.
Figure 1. Ineffective clearance of SARS-CoV-2 infection in the aged respiratory system.
So let’s first go through one of the figures—you’ll see figure one is a beautiful illustration drawn by my wonderful coauthors, Amber Mueller and Maeve McNamara. And it’s a picture of what goes wrong in the elderly compared to someone who can clear the infection. And what you’ll see is that there’s a cut through the lung. And what happens in the elderly is that the virus goes down into the lung, causes hyper immune response. And in the late stages of the disease in the elderly particularly, it’s a hyper immune response, which we call the cytokine storm. And what we’ve recently discovered, the planet that is not just my lab, is that the virus can attack the endothelial cells of the agent. And that’s not just in the lung, which of course is a problem for getting blood flow and oxygen across, but what’s also important is that these endothelial cells that line the blood vessels, particularly the micro capillaries, line at the heart, the brain, even the extremities.
And so what we’re seeing in elderly patients particularly that undergo this cytokine storm is what’s called a coagulopathy, which means that lining of the blood vessels is getting inflamed and causing clots to form. And you get a rise in this marker called the D-dimer, which is a breakdown product of clotting. And what we’re seeing is even in young people, there’s propensity for stroke, myocardial infarction, heart attack, and even things like numbing of the toes and the fingers. And you can see that there are what are called chilblains in some people, you get these dark areas on the body. So that’s particularly fatal if it’s not controlled and it’s very difficult to control that. So what’s behind all of this susceptibility to the agent?
Well, there are two things going on, mainly one is the inability to clear the virus initially. So if you’re young, you can have a spike in viral numbers. It starts to get in your throat, drift down into the lungs. But young people tend to not have this overreaction, they tend to form antibodies fairly rapidly and clear the viral. If you clear the virus very quickly, you’ll actually have very little risk of going into hospital or the ICU. As an aside, if you don’t have a very strong case of COVID-19, looks like you don’t mount a very strong immune response, but that’s another topic for a future discussion. What’s more important is to focus on: What is it about the aging immune system that’s defective that leads to their inability to clear the virus? And then the second part that’s important for the agent is: What happens once they start to clear the virus and why is that so detrimental?
And what we are seeing is that the virus particles, particularly the viral RNA, lasts a long time, sometimes for weeks in the body. And those remnants actually are what we think are stimulating this hyper-immune reaction cytokine storm, which is driven largely by a particular protein complex called the inflammasome, which is already hyperactive, chronically in the agent. And we’ll talk about that later on, but just to give a shout-out to my co-authors, their drawings were beautiful. So we’ll get back to the disease course in a moment. One of the things I want to bring up is one of the great things in this article that Amber and Maeve did was that they drew a table of respiratory viral infections and what are the risk factors? And so I have the table in front of me so I’ll just read off some of them, which you can see in the paper.
Mers in the original SARS, they actually had high risk. One of the risks was one in Type 2 diabetes, obesity, cardiovascular diseases, hypertension, old age, this is for Mers. For SARS one, it was again diabetes, renal disease, neurological diseases, metabolic, and interestingly dermatological diseases, which is probably an immune thing. But why is that important? What that tells us is that these particular type of corona viruses attack the agent, and in particular, the agent with underlying co-morbidities, these underlying diseases. But what I would like to us to consider and what I’d like to argue is that it’s not just about having obesity, having diabetes, having heart disease that is the problem. Those are symptoms of a more insidious problem, which is that those people are most likely older than their chronological age, or they’re actually very old biologically because they’ve lived a long time, but we know that biological age will be accelerated by being obese, by not exercising and just living the lifestyle that we know from epidemiology is not the perfect one.
At least half of America is overweight or obese. If you include certain cutoffs, some people estimate that it’s over 75% and this drives the aging process. And one of the side effects of course is obesity but obesity may not be the main driver actually, that’s a symptom of the problem that I want to talk to you about. So there are lots of things that go wrong in the aged body. And by age, I’m not just talking about birthday candles, I’m talking about actual biological age. Now biological age can be measured in a variety of ways. Let’s just talk about that for a minute. We can measure the DNA methylation status of ourselves, the so-called Horvath DNA methylation clock, we can measure that pretty easily in a blood test or a swab from the cheek these days get a very accurate estimation of how old someone is biologically.
But there are other things that change in a predictable way. And unlike 10 years ago where we thought we’d never have biomarkers, now we have quite a few. You can look at changes in immune cell diversity, such as T-cells, you can build a very good immune clock. You can look at the levels of NAD in the body, which decline with time. One of the things that we, Gordan Lauc and I, professor Gordan Lauc and I, wrote about is a paper actually also in the journal, Aging, is that the immune system changes in part because sugars change that are attached to proteins. This is the process of glycation and Gordan’s lab has done an amazing job, they’ve found that there’s a glycan clock and what he calls it is the glycogen age of a person.
And why is that important? Because as we get older, the type of sugars that are attached to proteins in the body, whether it’s antibodies or actually the coronavirus spike protein, and even the H2 so-called receptor on the surface of endothelial cells, these are all changed as we get older in terms of their glycation. And if you look at figure 3in the paper, you can see a beautiful rendition of these changes. And we also have epigenetic changes that control how cells behave. And we know that during aging, epigenetic changes occur, and we think that cells lose their identity. And that’s true for immune cells, it’s true for the lining of the blood vessels, the endothelial cells, and that may be why the virus has a greater chance of attacking an older person’s body as well.
And then finally, there’s the process of immunosenescence. Now that there’s two types of immunosenescence and I don’t want to get people confused here. Immunosenescence typically refers to just the aging of the overall immune system. That means that there’s less variety of T-cells. There’s less ability to mount an immune response and clear viruses, but there’s also cellular immunosenescence or what you call immuno. But there’s also cellular senescence which is a different story, which is about cells checking out of the cell cycle and becoming more like zombie cells. And you can stay in those for galactosidase or p16, and this is another type of cellular senescence.
There’s some overlap between the immunosenescence and cellular senescence, but it’s important to realize they’re not the same thing. And so that’s the lead-up to the whole paper, which goes into detail about these various causes susceptibility to viruses in general, but also to COVID-19. Now, one of the areas that we work on of course are the sirtuins. These are enzymes that our bodies make. There are seven of them in most of our cells, and they’re very important for fighting against diseases, both chronic diabetes, heart disease, Alzheimer’s, we believe based on a lot of mouse and human genetic studies. But also we’re finding are important for viral defenses. And we put forward a hypothesis in this paper that the sirtuin defenses are lost during COVID-19 infections. And one of the reasons for that is the following.
So sirtuins need NAD and unfortunately, as we get older, we think that a lot of our cells lose the ability to make an NAD effectively and they also destroy it for reasons that we don’t fully understand yet. But what we’ve also discovered in my lab and in others, Charlie Brenner put out a nice paper about this a few weeks ago, is that a virus, coronavirus and other types of viruses, deplete NAD in cells. And we think this is part of their defense, the viral attack and the inability of cells to survive the attack. Now they do this through activation of the PARPs. PARPs are poly ADP road to cell trans… polimeracion. So they do this by activating the PARPs, such as PARP1, PARP12, PARP14. And PARPs are enzymes that polymerize NAD and depleted from the cell. And we think that by either blocking the PARP activity or replacing, replenishing the NAD levels in infected cells and in the body of patients, we can give them a better chance of survival.
Now, why would we worry about NAD and sirtuins? Well sirtuins, particularly sirtuin 6, sirtuin 1, sirtuin 2, they control inflammation and they dampen it when it’s overactive. I mentioned the inflammasome. Well, one of the key components of the inflammasome is called NLRP3, and the acetylation chemical to that protein is what causes it to be active. Actually, if we deescalate of enzymes like CERT1, CERT2 deacetylate NLRP3, it brings that activity down. And so what we’re thinking is that when cells are infected, the NAD levels go down. So sirtuins are unable to dampen the inflammatory response and you get this cytokine storm. So in other words, if we were to raise NAD levels in patients, we may be able to prevent their bodies from going into this state of shock and aseptic like response.
Figure 2. Factors that increase the fatality risk of COVID-19.
Now I will admit, at first I didn’t think this was something that I should rush into. Of course, I would look like somebody with a hammer looking for a nail because you’d think that everything that I do looks like an NAD problem, but studies like the Brown paper that came out as well as studies over the last five years in my lab that have looked at NAD changes during macrophage activation and the PARP response have really pushed me into the belief that, as I write in this article with my coauthors, that NAD is part of this story. Now it’s not the whole story. In fact, the NAD story in this paper is only a small part of it, about 5%, but I want to talk about it because a lot of people are asking me, “David, what about NAD?” And interestingly, I’ve been working with a team in Boston on making an NAD precursor a drug.
And so for the last two years, with the help of a great team at Brigham and Women’s Hospital, they’ve been testing the safety and efficacy of an NAD precursor called MIB626, which is a proprietary version of NAD booster. So far, the molecule is extremely safe in the people that have been tested. It’s able to greatly raise NAD levels. Now there’s some debate out there in the Twitter-verse that the molecules that we work on in my lab and in these clinical trials don’t raise NAD and are not effective. Well, I can tell you that you probably shouldn’t get your scientific information from Twitter because it’s completely wrong. And now what’s interesting and exciting is that in the next few weeks, very extensive, double blind placebo controlled study is about to begin with this molecule. And we’ll see, pretty quickly I think, whether patients are helped by raising an NAD. Particularly the more severe ones.
Now, there are anecdotal case studies already. Some of them are online that you can look up if you’re interested, of patients recovering quite rapidly, supposedly, with treatment with NAD boosters like NMN, which is one of the ones that we work on. But those individual case studies don’t prove anything as we now know from having studied other molecules in other people’s study molecules in the world for COVID-19. So that’s why we’ve decided to do this very rigorous placebo controlled study and not just go for compassionate use. And we’ll see over the next few weeks, perhaps few months, realistically, whether this molecule that we’re working on is going to dampen the inflammatory response in patients that really need it. Drugs are very hard to make, most of them don’t work, so I’m not promising anything, I’m not expecting too much, but I think that we need to give this a shot.
And the other reason for believing in this work is that aging, as I started out in this review, in this talk mentioning, we think aging is the major driver of COVID-19 susceptibility. Aging of all of the different parts of the body in particular, the immune and circulatory systems. Now, if we can delay aging or reverse it, perhaps in some way with NAD boosting or with other drugs that are out there such as Metformin, which [inaudible] is arguing could be used to bring down blood sugar to improve the body’s survival. These kinds of longevity molecules could be used to bring not just the virus down, but boost the survival and the resilience and the defenses of the host up in the same way that you don’t just have weapons of war, you have the defenses as well.
And so on the defensive side, I think bringing up the defenses of the age is just as valid, if not more important than attacking the virus itself. So why would I say, “It’s just as important or more important?” Well consider that this is not the only virus that’s going to attack humanity going forward and vaccines while they’re great and we hold out full on. It probably won’t work against the next outbreak, whether it’s bird flu, regular flu, or another coronavirus, or even a mutated version of this one that’s out in the population. So we need to work also on the body’s ability to fight infections, in general.
So with that, I think I should let you all go. I’ve talked long enough about this paper. I hope you enjoy it. We really enjoyed writing it. It was challenging I’ll admit because it was written in real time as data was coming in and do a lot of things to update. And I’m grateful to Aging, the journal, for making papers available and published within rapid time. And I can tell you that the review process, the peer review process, was extensive. We’ve got pages and pages of comments from reviewers that really helped, particularly in this case. So, enjoy the paper and I’ll keep you updated through my other social media, but also through papers that we hope to publish in the next few months.
Thanks, take care.
Click here to read the full study published by Aging.
Aging is an open-access journal that publishes research papers monthly in all fields of aging research and other topics. These papers are available to read at no cost to readers on Aging-us.com. Open-access journals offer information that has the potential to benefit our societies from the inside out and may be shared with friends, neighbors, colleagues, and other researchers, far and wide.
Researchers from the Campisi Lab discovered new insights while investigating Cdkn1a transcript variants 1 and 2.
The Trending with Impact series highlights Aging publications that attract higher visibility among readers around the world online, in the news, and on social media—beyond normal readership levels. Look for future science news about the latest trending publications here, and at Aging-US.com.
—
Listen to an audio version of this article
The phenomenon in which cells are still metabolically active but can no longer proliferate is known as cellular senescence. Cellular senescence is a normal mechanism in development and tissue homeostasis—and a hallmark of aging.
“Our results are, to our knowledge, the first to study Ckdn1a transcript variants in the context of aging.”
THE STUDY
There are a number of mechanisms that drive cellular senescence. Previously, mRNA and protein coding gene Cdkn1a transcript variant 1 (p21var1) has been better-studied compared to Cdkn1a transcript variant 2 (p21var2). The authors of this paper explain that this is likely because the encoded protein is identical to that encoded by variant 1, and both variants are regulated by p53. However, neither variants have ever before been studied in the context of aging. In this study, the researchers explored the expression levels of both Cdkn1a transcript variants 1 and 2 in the context of cellular senescence using several tissues from aged mice and a cell culture model of mouse cells.
“The stringent cell growth arrest associated with cellular senescence is determined, among other mechanisms, by activities of cyclin-dependent kinase inhibitor proteins p16Ink4a and p21Cip1/Waf1, encoded by the Cdkn2a and Cdkn1a loci, respectively [1].”
Study results showed that both variants are induced during cellular senescence. They showed that p21var1 and p21var2 are equally sensitive to transcriptional upregulation after p53 stabilization. The in vitro models also found that p21var2 is preferentially induced with age.
“In sum, p21var2 expression is consistently elevated with age, in contrast with an absence of age-related change in p21var1 levels.”
The researchers conducted further tests in vivo to examine the expression pattern of p21var2 and their results suggested that the circadian regulation of p21Cip1/Waf1 is driven solely by expression of Cdkn1a transcript variant 1. The team also induced cellular senescence in vivo with doxorubicin and ABT-263 (navitoclax) and evaluated the variants’ expression. These results confirmed their in vitro findings that p21var2 is more prone to cellular senescence than p21var1, thus making it a better marker for assessing the presence of senescent cells in vivo.
CONCLUSION
“We show that, although tissue-specific exceptions may arise, p21var2 but not p21var1 is a better candidate marker of aging and senescence in mice.”
Click here to read the full research paper, published by Aging.
Aging is an open-access journal that publishes research papers monthly in all fields of aging research and other topics. These papers are available to read at no cost to readers on Aging-us.com. Open-access journals offer information that has the potential to benefit our societies from the inside out and may be shared with friends, neighbors, colleagues, and other researchers, far and wide.
Behind the Study is a series of transcribed videos from researchers elaborating on their recent oncology-focused studies published by Aging. A new Behind the Study is released each Monday. Visit the AgingYouTube channel for more insights from outstanding authors.
—
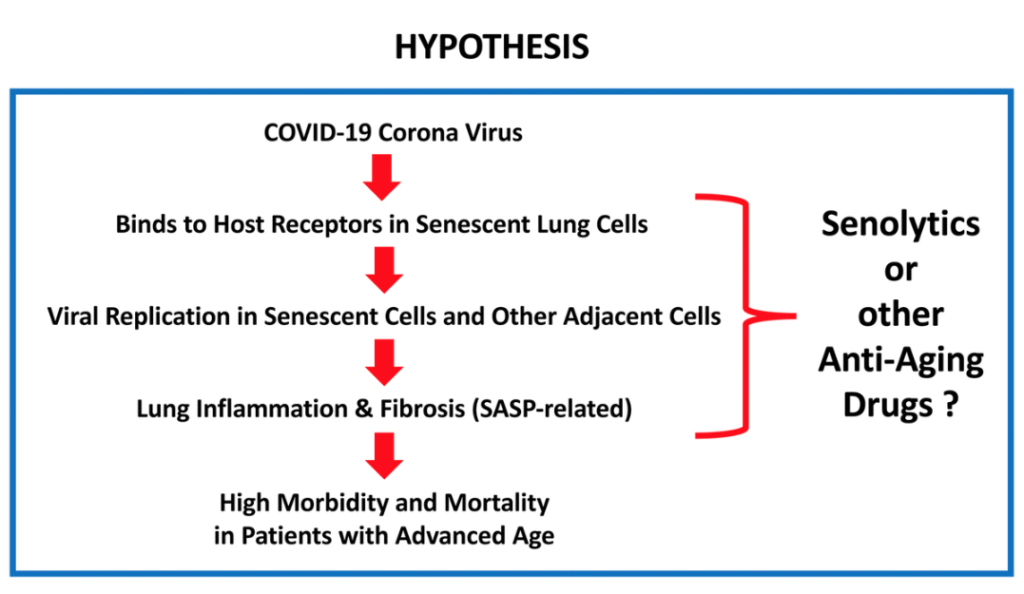
Hi, I’m professor Michael Lisanti and I’m the Chair of Translational Medicine at the University of Salford, and today I want to talk about our new prospective article, which links COVID-19 and chronological aging, and is focused on potential treatments and prevention strategies. I got interested in this topic because there seems to be an association between COVID-19 fatalities and aging, especially in patients with advanced chronological age. Patients over 65, and their 70s and 80s, are more likely to have increased morbidity and mortality. And so, I thought there may be a link there, between aging and senescence and the viral replication, as well as the potential therapy.
What I’d like to highlight about this particular article is that it proposes potential treatment strategies as well as prevention strategies. The reason is because it appears that this disease, the virus itself, may target senescent cells and senescent cells have been rewired to increase protein synthesis and also to increase the secretion of inflammatory mediators, which is known as the SASP, the senescence-associated secretory phenotype.
And so, one idea would be to use drugs that are senolytics. Senolytics are drugs that target and lyse senescent cells, but also to use protein synthesis inhibitors. The reason is because proteins synthesis inhibitors and senolytic drugs would prevent viral replication, which would reduce viral transmission. And so this could be used as a preventative strategy. I’ll just give you a couple of examples. If you have a drug which is an FDA-approved protein synthesis inhibitor, it should inhibit the secretion of inflammatory mediators, like IL-6. It should inhibit the fibrosis by preventing the secretion and production of collagen. And most importantly, the virus is also made of protein, so if you have a protein synthesis inhibitor, it will also inhibit viral replication.
Figure 1.What is the relationship between COVID-19 and advanced chronological age?
There are three drugs I’d like to mention in particular. One is azithromycin, which is a senolytic. The others are also protein synthesis inhibitors, like doxycycline and rapamycin. All three have been shown to reduce IL-6 production because of their inhibition of protein synthesis activity. And also, all three of them have been shown to inhibit viral replication, not specifically of COVID 19, but since this effect on protein synthesis is a generalized effect, it should work for any virus. For example, azithromycin has been shown to inhibit the replication of Zika virus and Ebola virus, doxycycline has been shown to inhibit the replication of dengue virus, and rapamycin, which is another protein synthesis inhibitor with anti-aging properties, has been shown to inhibit replication of the HIV virus.
So, it seems to me that it’s a no-brainer that we should be repurposing FDA-approved drugs that are protein synthesis inhibitors, both for prevention, to prevent the inflammation fibrosis that’s occurring that’s killing people with COVID-19, and also to prevent the contagion by inhibiting viral replication. So I think this could provide a very inexpensive way forward because drugs like doxycyclin are only less than 10 cents a day, and could be used, as I said, for both prophylaxis and treatment. But, I think we need to use it early in the disease to prevent the fibrosis and inflammation, which makes them long, very inflexible and unable to expand and contract, and leads them to a fibrotic lung disease, which prevents patient recovery and could explain lethality of the disease.
I would like to directly engage with people to pick this up, to bring this forward as potential clinical trials. These clinical trials could be done directly in healthcare workers because they are the most vulnerable. In addition, they could be done in patients with advanced chronological age, or even with patients that are asymptomatic, that have been identified as the virus-positive. And it would be like a window trial where you would do viral titers first, and then you would give the drug and then you could also look at the viral titers after administering the drugs. So this would be a very easy, straightforward trial.
All the diagnostic tools for COVID-19 have already been identified and perfected, so all we need to do is interject FDA-approved drugs, which are protein synthesis inhibitors, to look at the eradication, the virus. So this would also be a very inexpensive clinical trial. But I would like to engage with infectious disease experts and virologists to help facilitate. Thank you.
Of course, I would like to thank two foundations which have supported our work: The Fox Point Foundation in Canada and The Healthy Life Foundation in the UK for providing the equipment and infrastructure at the University of Salford.
Click here to read the full paper, published by Aging.
Aging is an open-access journal that publishes research papers monthly in all fields of aging research and other topics. These papers are available to read at no cost to readers on Aging-us.com. Open-access journals offer information that has the potential to benefit our societies from the inside out and may be shared with friends, neighbors, colleagues, and other researchers, far and wide.
In 2018, Dr. Mikhail Blagosklonny wrote a thought provoking theory article, entitled: “Disease or not, aging is easily treatable.”
Figure 1. Relationship between aging and diseases. When growth is completed, growth-promoting pathways increase cellular and systemic functions and thus drive aging. This is a pre-pre-disease stage, slowly progressing to a pre-disease stage. Eventually, alterations reach clinical disease definition, associated with organ damage, loss of functions (functional decline), rapid deterioration and death.
The Top-Performer series highlights papers published by Aging that have generated a high Altmetric attention score. Altmetric scores, located at the top-left of trending Aging papers, provide an at-a-glance indication of the volume and type of online attention the research has received.
Would re-classifying aging as an official disease help fuel the anti-aging drug industry? While many sufficient arguments can place aging in this category, Dr. Mikhail Blagosklonny—Editor-in-Chief at Aging, Oncotarget, Oncoscience, and Cell Cycle, and adjunct faculty member at the Roswell Park Comprehensive Cancer Center—believes that classifying aging as a disease is unnecessary and counterproductive.
“It is commonly argued that aging should be defined as a disease so as to accelerate development of anti-aging therapies. This attitude is self-defeating because it allows us to postpone development of anti-aging therapies until aging is pronounced a disease by regulatory bodies, which will not happen soon.”
In this article, Dr. Blagosklonny emphasizes his theory that human aging is the quasi-programmed continuation of growth and development. He explains that progressive aging later in life results in aberrant systematic hyperfunction, which leads to disease and, eventually, death.
“Aging is a normal continuation of the normal developmental program, so it is NOT a program but a purposeless, unintended quasi-program [10–16].”
Beginning after the growth process, Dr. Blagosklonny segments the aging process into four stages: pre-pre-disease, pre-disease, clinical disease, and death (see Figure 1). In the early stages of aging, the unseen asymptomatic abnormalities which arise have not yet reached the currently agreed upon clinical definitions of disease. Dr. Blagosklonny explains that “healthy” aging can be interchangeable with “pre-pre-disease” and “pre-disease.”
“‘Healthy’ aging has been called subclinical aging [33], slow aging [18,34] or decelerated aging [35], during which diseases are at the pre-disease or even pre-pre-disease stage.”
TREATING AGING
“Aging is easily treatable.”
Dr. Blagosklonny justifies this instinctually debatable claim simply by pointing out the ways in which humans are already defying aging. Calorie restriction, intermittent fasting, and the ketogenic diet have all been proven to slow aging and extend healthy lifespan. Certain nutrients, conventional drugs, and pharmacological therapies which have shown anti-aging properties include metformin, aspirin, statins, beta-blockers, ACE inhibitors, Angiotensin II receptor blockers (ARB), and (the anti-aging therapy Dr. Blagosklonny is most intrigued by) rapamycin, and other rapalogs.
“Rapamycin (Rapamune/Sirolimus), an allosteric inhibitor of mTOR complex 1 [63,66], is a natural rapalog as well as the most potent and best studied rapalog.”
Dr. Blagosklonny chronicles numerous studies over the years verifying rapamycin’s life- and health-extending effects in microorganisms, mice, humans, (non-human) primates, and even canines. Read more about the origin and applications of rapamycin.
PREVENTATIVE MEDICINE IS ANTI-AGING
“Gerontologists think of metformin as an anti-aging drug [121–130], and metformin can be combined with rapamycin [131].”
In addition to the use of rapamycin and other anti-aging drugs, current preventative medicine strategies can be seen as anti-aging therapies, and vice versa. Dr. Blagosklonny discusses examples of preventative medicine and anti-aging therapy. In one example, patients who present with pre-diabetic symptoms may be treated with metformin to decrease insulin-resistance in advance, in order to prevent diabetes in the future. This is an example of preventative medicine as an anti-aging therapy.
“Physicians generally do not think of metformin as an anti-aging drug, simply because it is expected that life will be extended, if diseases are prevented.”
CONCLUSION
“Aging does not need to be defined as a disease to be treated.”
In conclusion, Dr. Blagosklonny proposes that “aging can be treated as a pre-disease to prevent its progression to diseases.” He suggests that, to preventatively combat disease brought on by aging, rapamycin and conventional life-extending drugs can be combined with “modestly low-calorie/carbohydrates diet, physical exercise, and stress avoidance.”
Click here to read the full theory article, published by Aging.
Aging is an open-access journal that publishes research papers monthly in all fields of aging research and other topics. These papers are available to read at no cost to readers on Aging-us.com. Open-access journals offer information that has the potential to benefit our societies from the inside out and may be shared with friends, neighbors, colleagues, and other researchers, far and wide.
In a trending Aging editorial paper, researchers explain that switches in the aging process may be a window of opportunity for patients with Alzheimer’s disease and potential epigenetic treatments.
Figure 1. The EORS downward spiral of aging and Alzheimer’s (Epigenetic Oxidative Redox Shift) [2].
The Trending with Impact series highlights Aging publications that attract higher visibility among readers around the world online, in the news, and on social media—beyond normal readership levels. Look for future science news about the latest trending publications here, and at Aging-US.com.
—
Listen to an audio version of this article
Alzheimer’s disease (AD) develops at different times for different people due to known and unknown variables. AD and aging share a number of features in common, such as oxidative stress, mitochondrial impairment, and bioenergetic and metabolic shifts. Aging is an unmistakable risk factor for Alzheimer’s disease, but what causes aging to switch it on? Do these “switches” present opportunities for intervention?
“[…] the complex mechanisms of switching on so many AD pathologies remain underexplored.”
Oxidative Shifts
“Age-related redox stress, often measured as oxidative stress in aging and AD launches a global switch in the epigenetic landscape, widely affecting methylation, histone modification, and noncoding RNA regulation [5], to further drive downstream metabolic and energetic shifts.”
The authors begin this editorial paper by prefacing readers with the epigenetic oxidative redox shift theory of aging. They explain that the sedentary lifestyle often accompanied by old age resets epigenetic marks to prepare for low mitochondrial capacity and minimal energy production. In order to maintain this setting (resting redox energy levels), the body switches to require more oxygen and energy when performing physical activities and increases the conversion of glucose to lactose (the Warburg Effect). In turn, these metabolic shifts (now enforced by the epigenome) reinforce sedentary behavior—forming a vicious cycle.
“Our environment, lifestyle, stress, physical activity, and habits all modulate epigenetic control of gene expression for continuous environmental tracking.”
Conclusion
Oxidative shifts alter the activity of numerous redox-sensitive transcription factors, enzymes, and signaling proteins. The researchers explain that these oxidative switches taking place in patients with Alzheimer’s disease are potential targets for epigenetic treatments.
“While studies on these ‘switches’ enable elucidation of the underlying mechanisms for when aging switches on Alzheimer’s degeneration, more importantly, these ‘switches’ of redox, epigenetics and neuroinflammation encourage early interventions to decelerate AD pathology and retain functional memory.”
Click here to read the full paper, published by Aging.
Aging is an open-access journal that publishes research papers monthly in all fields of aging research and other topics. These papers are available to read at no cost to readers on Aging-us.com. Open-access journals offer information that has the potential to benefit our societies from the inside out and may be shared with friends, neighbors, colleagues, and other researchers, far and wide.














![Figure 1. The EORS downward spiral of aging and Alzheimer’s (Epigenetic Oxidative Redox Shift) [2].](/wp-content/uploads/2021/06/Screen-Shot-2021-06-24-at-4.27.37-PM-1024x636.png)